REITER'S
ARTHRITIS:
REITER'S
ARTHRITIS:
1. Distribution:
The MTP joints, first IP, and the calcaneus are the most frequently involved
joints in the foot. Initially there is a monoarticular involvement which may
lead to the misdiagnosis of septic arthritis. The calcaneus is involved in
50% of patients.
2. Erosion pattern:
Like psoriatic arthritis, ill-defined erosions with uniform joint loss and
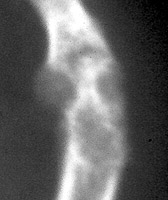
bone proliferation are observed. In addition, periostitis along bone shafts
is present. There may be fusiform soft tissue swelling involving a single
digit, giving appearance of a sausage. Early juxta-articular osteoporosis
is present however there is usually a re-establishment of normal mineralization.There
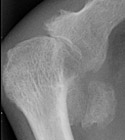
is erosion and bone production at the attachment of the Achilles tendon and
the plantar aponeurosis. Soft tissue swelling and fluffy periostitis involving
the distal ends of the tibia and fibula are characteristic for ankle involvement.
3. Differential diagnosis:
Radiographic changes characteristic of arthritis of Reiter's disease are identical
to those of psoriatic arthritis. However, the differences in distribution
between the two allows for more accurate diagnosis. Reiter's arthritis predominately
involves lower extremity, primarily feet, ankles, knees, and SI joints in
bilateral asymmetric distribution. Hands, hips, and spine are less frequently
involved.