The Symes amputation can be one of the best amputation of the lower extremity. When
it is done right, it creates an excellent end-bearing stump and allows for a
functionally most satisfactory prosthesis. When is is done badly, the procedure is
useless and the patient must be amputated at a higher level. Problems include
posterior migration of the heel pad, skin slough, and a distal flair that leads to a bulky
and thus non-cosmetically pleasing prosthesis. The level of
the amputation in generally at the distal tibia and fibula 0.6cm proximal to the periphery
of the ankle joint and passing through the dome of the ankle centrally. In the past,
the Symes amputation was less used for ischemic limbs because of poor wound healing at
this level. However, newer techniques for determination of tissue perfusion such as
Doppler ultrasound measurement of segmental blood pressures, radioactive xenon clearance
tests, and transcutaneous oxygen measurements have significantly increased the success
rate of the Symes amputation in these limbs.
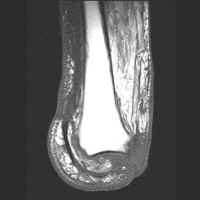
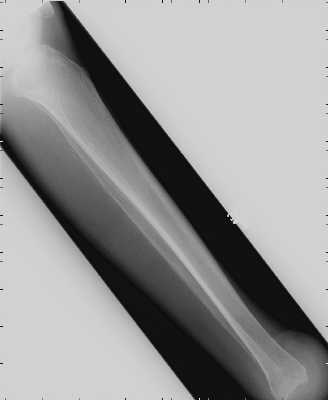
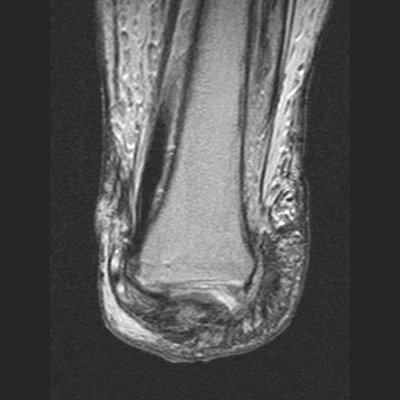
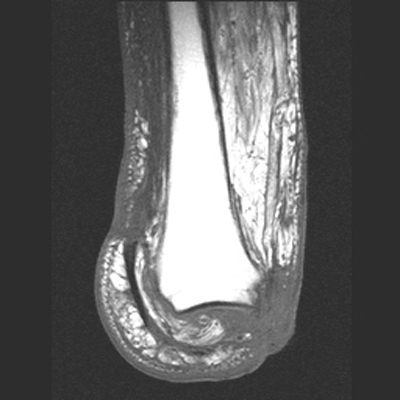
The MRI images below demonstrate the level of the Symes amputation along with bony and
soft tissue changes. Note the thick heel pad forming the majority of the distal
stump: the principle advantage of this procedure due to the more effective weight bearing.